


Human immunodeficiency virus (HIV) infection is a viral infection that progressively destroys certain white blood cells and is treated with antiretroviral medications. If untreated, it can cause acquired immunodeficiency syndrome (AIDS), which is sometimes referred to as end-stage HIV infection.
HIV is transmitted through exchange of bodily fluids (semen, vaginal fluid, blood, breast milk) with an infected person, usually through vaginal or anal sex, sharing needles, or from mother to child (during pregnancy, birth, or breastfeeding).
HIV destroys certain types of white blood cells, weakening the body’s defenses against infections and cancers.
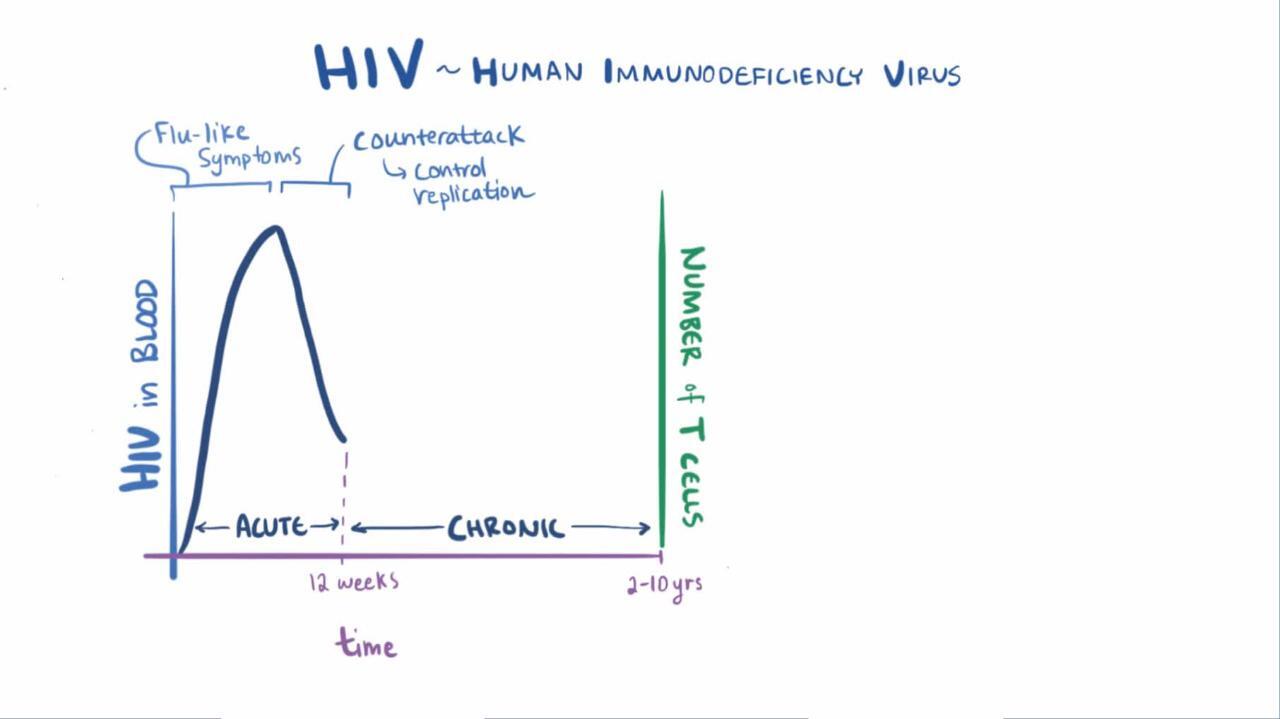
When people are first infected, symptoms of fever, rashes, swollen lymph nodes, and fatigue may last a few days to several weeks, and then they may have no symptoms for more than a decade.
Blood tests to check for HIV antibody and to measure the amount of HIV virus can confirm the diagnosis.
HIV screening tests are available for adults and adolescents, particularly pregnant women regardless of what their risk appears to be.
HIV medications (antiretroviral medications) can stop HIV from reproducing, allow the immune system to strengthen, and thus allow people to live without severe infections or HIV-related cancers.
Most untreated people eventually become ill and develop AIDS, defined by the presence of serious infections and cancers.
(See also HIV Infection in Children.)
HIV infections may be caused by 1 of 2 retroviruses, HIV-1 or HIV-2 (see sidebar What Is a Retrovirus?). HIV-1 causes most HIV infections worldwide, but HIV-2 causes many HIV infections in West Africa. HIV-2 appears to be less severe than HIV-1.
Infection with another type of retrovirus, human T-lymphotropic virus 1 (HTLV-1), is less common but can also cause serious disease.
HIV progressively destroys certain types of white blood cells called CD4+ lymphocytes. Lymphocytes help defend the body against foreign cells, infectious organisms, and cancer. Thus, when HIV destroys CD4+ lymphocytes, people become susceptible to attack by many other infectious organisms. Many of the complications of HIV infection, including death, usually result from these other infections and not from HIV infection directly.
HIV-1 originated in Central Africa during the first half of the 20th century, when a closely related chimpanzee virus first infected people. The global spread of HIV-1 began in the late 1970s, and AIDS was first recognized in 1981.
As of 2021, an estimated 29.6 million people with HIV were accessing antiretroviral therapy (up from 7.8 million in 2010) as the result of international efforts, which led to dramatic reductions in deaths and transmission in many countries.
In the United States at the end of 2021, an estimated 1.2 million people aged 13 years or older were estimated to have HIV infection, including an estimated 153,500 (13%) people whose infections had not been diagnosed. In 2022, over 32,100 people received an HIV diagnosis, and 22,400 cases were due to male-to-male sexual contact. Data for 2020 should be interpreted with caution due to the lingering impact of the COVID-19 pandemic on access to HIV testing, care-related services, and case surveillance activities.
In 2022, worldwide HIV statistics showed that approximately
39 million people, including 1.5 million children under age 15, had HIV infection.
1.3 million people were newly diagnosed with HIV, down from 2.1 million in 2010.
630,000 people died from HIV-related illnesses, compared to 1.3 million in 2010.
29.8 million people with HIV received antiretroviral therapy.
86% of people with HIV knew their status (76% of those who knew their status are receiving treatment and 71% have suppressed viral loads)
HIV infection is most prevalent in Africa, particularly in sub-Saharan Africa. WHO estimated 2022 statistics in Africa show that approximately
25.6 million had HIV infection (90% knew their status, 82% were receiving treatment, and 76% had suppressed viral loads).
660,000 people were newly diagnosed with HIV infection (a 66% decrease in incidence from 2010).
380,000 people died from HIV-related causes (a 56% decrease from 2010).
Upungufu wa Kinga Mwilini (UKIMWI)
AIDS (or end-stage HIV infection) is the most severe form of HIV infection. HIV infection is considered to be end-stage when at least one serious complicating illness develops or the number (count) of CD4+ lymphocytes decreases substantially.
When people who are infected with HIV develop certain illnesses, end-stage HIV infection is diagnosed. These illnesses, called AIDS-defining illnesses, include
Serious infections that occur mainly in people with a weakened immune system (called opportunistic infections), including fungal infections (such as cryptococcosis and Pneumocystis jirovecii pneumonia), bacterial infections (such as Mycobacterium avium complex and Mycobacterium tuberculosis), and viral infections (such as severe herpes simplex infections and cytomegalovirus infections)
Certain cancers, such as invasive cervical cancer, Kaposi sarcoma, and certain lymphomas
Dysfunction of the nervous system
A substantial loss of weight due to HIV infection (AIDS wasting)
Uenezaji wa Maambukizi ya VVU
The transmission of HIV requires contact of an open surface (such as a cut) in an uninfected person with a body fluid that contains the virus. HIV can appear in nearly any body fluid, but transmission occurs mainly through blood, semen, vaginal fluid, and breast milk. Although tears, urine, and saliva may contain low concentrations of HIV, transmission through these fluids is extremely rare, if it occurs at all.
HIV is not transmitted by contact that does not involve exchange of body fluids (such as touching, holding, or dry kissing) or by close, nonsexual contact (such as touching a surface or an object). No case of HIV transmission has been traced to the coughing or sneezing of an infected person or to a mosquito bite. Transmission from an infected doctor or dentist to a patient is extremely rare.
HIV is usually transmitted in the following ways:
Sexual contact with an infected person, when the mucous membrane lining the mouth, vagina, penis, or rectum is exposed to body fluids such as semen or vaginal fluids that contain HIV, as occurs during unprotected sexual intercourse
Injection of contaminated blood, as can occur when needles are shared or a health care worker is accidentally pricked with an HIV-contaminated needle
Transfer from an infected mother to a child before birth, during birth, or after birth through the mother’s milk
Medical procedures, such as transfusion of blood that contains HIV, procedures done with inadequately sterilized instruments, or transplantation of an infected organ or tissues
HIV is more likely to be transmitted if skin or a mucous membrane is torn or damaged—even if minimally. During vaginal or anal sex, small cuts may occur in the genitals or surrounding skin, even if the person is not aware that a cut is present.
Most HIV infections are transmitted through heterosexual contact, but risk factors vary according to region or national income levels. For instance, transmission among men who have sex with men is usually the most common way infection occurs in high-resource countries, but people who inject drugs are disproportionally affected in Central and Eastern.
In areas where heterosexual transmission is dominant, HIV infection follows routes of trade, transportation, and economic migration to cities and spreads secondarily to rural areas.
Transmission of HIV through its most common routes—sexual contact or sharing of needles—is almost completely preventable.
Did You Know...
|
Kupitia shughuli ya ngono
Risk of transmitting HIV is highest during vaginal or anal sex when a condom is not used or is used incorrectly. HIV transmission can also occur during oral sex, although transmission is less likely than during vaginal or anal sex. However, open sores in the mouth, vagina, penis, or rectum, bleeding gums, and oral contact with menstrual blood may increase the risk.
Risk of HIV infection is increased when semen or vaginal fluids contain a large amount of HIV and/or when there are tears or sores, even small ones, in the skin or membranes lining the genitals, mouth, or rectum. Thus, transmission is much more likely during the following:
The first weeks after people are infected because at that time, the blood and body fluids contain very large amounts of HIV
Vigorous sexual activities that damage the skin or membranes lining the genitals, mouth, or rectum
Sexual intercourse when either partner has a genital herpes infection, syphilis, or another sexually transmitted infection (STI) that can cause sores or tears in the skin or inflammation of the genitals
HIV (antiretroviral) medications can reduce the amount of HIV in semen and vaginal fluids. Thus, treatment of HIV infection with these medications can significantly reduce the likelihood of transmission.
Sexual activities that can damage the membranes lining the genitals, mouth, or rectum include fisting (inserting most or all of the hand into the rectum or vagina) and using sex toys.
Studies show that people with HIV infection who are treated with antiretroviral therapy and have an undetectable viral load (virally suppressed) do not sexually transmit the virus to their partners.
What Is the Risk of HIV Transmission During Sexual Activities?
Risk | Activity |
|---|---|
None (unless sores are present) | Dry kissing Body-to-body rubbing and massage Use of inserted sexual devices (for example, sex toys) that are not shared with others Stimulation of the genitals by a partner if there is no contact with semen or vaginal fluids Bathing or showering together Contact with feces or urine if the skin is intact |
Theoretical (extremely low risk unless sores are present) | Wet kissing Oral sex done to a male (fellatio) if ejaculation does not occur or a condom is used Oral sex done to a female (cunnilingus) if a barrier is used Oral-anal contact Vaginal or anal penetration by a hand with or without a glove Use of inserted sexual devices/toys that are shared but are disinfected |
Low | Oral sex done to an infected male with or without ingestion of semen if a condom is not used or is used incorrectly (risk is less if oral sex is done to an uninfected male by an infected person) Oral sex done to a female if no barrier is used Vaginal or anal intercourse if a condom is used correctly (for example, using only water-based lubricants and not spilling any semen) Use of inserted sexual devices/toys that are shared but are not disinfected |
High | Vaginal or anal intercourse with or without ejaculation if a condom is not used or is used incorrectly |
Kupitia kwenye sindano au vifaa vingine
Health care workers who are accidentally pricked with an HIV-contaminated needle have approximately a 1 in 400 chance of contracting HIV unless they are treated as soon as possible after exposure. Such treatment reduces the chance of infection. The risk increases if the needle penetrates deeply or if the needle is hollow and contains HIV-contaminated blood (as with a needle used to draw blood or to inject illicit drugs) rather than simply being coated with blood (as with a needle used to stitch a cut).
Infected fluid splashing into the mouth or eyes has less than a 1 in 1,000 chance of causing infection.
Kutoka kwa mama hadi mtoto
HIV infection in a large number of women of childbearing age has led to an increase in HIV infection among children.
HIV infection can be transmitted from a mother infected with HIV to her child in the following ways:
During pregnancy, to the fetus through the placenta
During childbirth, to the baby during passage through the birth canal
To the baby after birth through breast milk
The overall cumulative risk of transmission from mother to child without antiretroviral medications is 35 to 45%.
Treating infected pregnant women with antiretroviral medications can significantly reduce the risk of transmission. Women who are pregnant and infected with HIV should be treated during the second and third trimesters of pregnancy, during delivery, and during breastfeeding. Doing a cesarean delivery and treating the baby for several weeks after birth also reduce the risk.
HIV is excreted in breast milk. Mothers infected with HIV should not breastfeed if they live in areas where formula feeding is safe and affordable. However, in areas where infectious diseases and undernutrition are common causes of infant death and where safe, affordable infant formula is not available, the World Health Organization recommends antiretroviral treatment combined with breastfeeding for at least 12 months. In such cases, the protection provided by breastfeeding from potentially fatal infections may counterbalance the risk of HIV transmission.
Because many women with HIV infection and their infants are treated or take medications to prevent HIV infection, the number of children getting HIV is decreasing in many countries.
Kupitia kuongezewa damu au vipandikizi vya kiungo
Currently, HIV infection is rarely transmitted through blood transfusions or organ transplants.
Since 1985 in most high-resource countries, all blood collected for transfusion has been tested for antibodies to HIV and HIV RNA. When possible, some blood products are treated with heat to eliminate the risk of HIV infection. The current risk of HIV infection from a single blood transfusion (which is carefully screened for HIV and other bloodborne viruses) is estimated to be less than 1 in about 2 million in the United States. However, in many l countries where blood and blood products are not screened for HIV or are not screened as stringently, the risk of bloodborne HIV infection remains substantial.
HIV has been transmitted when organs (kidneys, livers, hearts, pancreases, bone, and skin) from infected donors were unknowingly used as transplants. HIV transmission is unlikely to occur when corneas or certain specially treated tissues (such as bone) are transplanted.
Kupandikiza kwa njia ya bandia
HIV transmission is also possible when sperm from an infected donor is used for insemination. In the United States, measures have been taken to reduce this risk. Fresh semen samples are no longer used. Sperm from donors is frozen for 6 months or more. Then the donors are retested for HIV infection before the sperm is used.
If a sperm donor is known to have HIV infection, washing sperm is an effective way to remove HIV from sperm.
Utaratibu wa maambukizi ya Virusi Vya Ukimwi
Once in the body, HIV attaches to several types of white blood cells. The most important are certain helper T lymphocytes (T cells). Helper T lymphocytes activate and coordinate other cells of the immune system. On their surface, these lymphocytes have a receptor called CD4, which enables HIV to attach to them. Thus, these helper lymphocytes are designated as CD4+.
HIV is a retrovirus. That is, it stores its genetic information as ribonucleic acid (RNA). Once inside a CD4+ lymphocyte, the virus uses an enzyme called reverse transcriptase to make a copy of its RNA, but the copy is made as deoxyribonucleic acid (DNA). HIV mutates easily at this point because reverse transcriptase is prone to making errors during the conversion of HIV RNA to DNA. These mutations make HIV more difficult to control because the many mutations increase the chance of producing HIV that can resist attacks by the person’s immune system and/or antiretroviral medications.
The HIV DNA copy is incorporated into the DNA of the infected lymphocyte. The lymphocyte’s own genetic machinery then reproduces (replicates) the HIV. Eventually, the lymphocyte is destroyed. Each infected lymphocyte produces thousands of new viruses, which infect other lymphocytes and destroy them as well. Within a few days or weeks, the blood and genital fluids contain a very large amount of HIV, and the number of CD4+ lymphocytes may be reduced substantially. Because the amount of HIV in blood and genital fluids is so large so soon after HIV infection, newly infected people transmit HIV to other people very easily.
Simplified Life Cycle of the Human Immunodeficiency Virus
Like all viruses, human immunodeficiency virus (HIV) reproduces (replicates) using the genetic machinery of the cell it infects, usually a CD4+ lymphocyte.
Medications used to treat HIV infection were developed based on the life cycle of HIV. These medications inhibit the 3 enzymes (reverse transcriptase, integrase, and protease) that the virus uses to replicate or to attach to and enter cells. |


When HIV infection destroys CD4+ lymphocytes, it weakens the body’s immune system, which protects against many infections and cancers. This weakening is part of the reason that the body is unable to eliminate HIV infection once it has started. However, the immune system is able to mount some response. Within a month or two after infection, the body produces lymphocytes and antibodies that help lower the amount of HIV in the blood and keep the infection under control. For this reason, untreated HIV infection may cause no symptoms or only a few mild symptoms for an average of about 10 years (ranging from 2 to more than 15 years).
HIV also infects other cells, such as cells in the skin, brain, genital tract, heart, and kidneys, causing disease in those organs.
Idadi ya CD4
The number of CD4+ lymphocytes in blood (the CD4 count) helps determine the following:
How well the immune system can protect the body from infections
How severe the damage done by the HIV is
Most healthy people have a CD4 count of 500 to 1,000 cells per microliter of blood. Typically, the number of CD4+ lymphocytes is reduced during the first few months of infection. After about 3 to 6 months, the CD4 count stabilizes, but without treatment, it usually continues to decline at rates that vary from slow to rapid.
If the CD4 count falls below about 200 cells per microliter of blood, the immune system becomes less able to fight certain infections (such as Pneumocystis jirovecii pneumonia). Most of these infections are rare in healthy people. However, they are common among people with a weakened immune system. Such infections are called opportunistic infections because they take advantage of a weakened immune system.
A count below about 50 cells per microliter of blood is particularly dangerous because additional opportunistic infections that can rapidly cause severe weight loss, blindness, or death commonly occur. These infections include
kiwango cha virusi
The amount of HIV in the blood (specifically the number of copies of HIV RNA) is called the viral load.
Viral load represents how quickly HIV is replicating. When people are first infected, the viral load increases rapidly. Then, after about 6 months, even without treatment, it drops to a lower level, which remains constant, called the set point. This level varies widely from person to person—from as little as a few hundred to over a million copies per microliter of blood.
Viral load also indicates
How contagious the infection is
How fast the CD4 count is likely to decrease
How fast symptoms are likely to appear
The higher the set point of the viral load, the more quickly the CD4 count decreases to the low levels (less than 200) that increase risk of opportunistic infections, even in people without symptoms.
During successful treatment, the viral load decreases to very low or undetectable levels (less than about 20 to 40 copies per microliter of blood). However, inactive (latent) HIV is still present within cells, and if treatment is stopped, HIV starts replicating and the viral load increases.
An increase in the viral load during treatment may indicate the following:
The HIV has developed resistance to antiretroviral treatment.
The person is not taking the prescribed medications.
Both
Did You Know...
|
Dalili za maambukizi ya virusi vya Ukimwi
Maambukizi ya kwanza
When initially infected, many people have no noticeable symptoms, but within 1 to 4 weeks, fever, rashes, sore throat, swollen lymph nodes, fatigue, and a variety of less common symptoms develop in some people. Symptoms of initial (primary) HIV infection usually last from 3 to 14 days.
Kipindi cha dalili kiasi au cha bila dalili
After the first symptoms disappear, most people, even without treatment, have no symptoms or only occasionally have a few mild symptoms. This interval of few or no symptoms may last from 2 to 15 years. The symptoms that most commonly occur during this interval include the following:
Swollen lymph nodes, felt as small, painless lumps in the neck, under the arms, or in the groin
White patches in the mouth (thrush) due to candidiasis (a yeast infection)
Diarrhea
Fatigue
Fever sometimes with sweating
Progressive loss of weight
Anemia
Some people progressively lose weight and have a mild fever or diarrhea.
These symptoms may result from HIV infection or from opportunistic infections that develop because HIV has weakened the immune system.
Dalili kali zaidi
For some people, the first symptoms are those of AIDS.
AIDS (also referred to a end-stage HIV infection) is defined as the development of very serious opportunistic infections or cancer—the ones that usually develop only in people with a CD4 count of less than 200 cells per microliter of blood.
The specific opportunistic infections and cancers that develop cause many of the symptoms. These infections occur more frequently or are more severe in people with HIV infection than in those without the infection.
Serious opportunistic infections may cause various symptoms depending on the organ affected:
Lungs: Fever, cough, or shortness of breath
Brain: Headache, weakness, loss of coordination, or deterioration of mental function
Digestive tract: Pain, diarrhea, or bleeding
HIV can also cause symptoms when it directly infects and damages organs such as the following:
Brain: Brain damage with memory loss, difficulty thinking and concentrating, or both, eventually resulting in dementia if HIV infection is not treated, as well as weakness, tremor, or difficulty walking
Kidneys: Kidney failure with swelling in the legs and face, fatigue, and changes in urination, but often not until the infection is severe
Heart: Heart failure with shortness of breath, cough, wheezing, and fatigue (uncommon)
Genital organs: Decreased levels of sex hormones, which may cause fatigue and sexual dysfunction in men
HIV is probably directly responsible for a substantial loss of weight (AIDS wasting) in some people. Wasting in people with AIDS may also be caused by a series of infections or by an untreated, persistent digestive tract infection.
Common Opportunistic Infections Associated With AIDS
Infection | Description | Symptoms |
|---|---|---|
A yeast infection of the esophagus | Painful swallowing and burning in the chest | |
An infection of the lungs with the fungus Pneumocystis jirovecii | Difficulty breathing, cough, and fever | |
Infection with the parasite Toxoplasma gondii, usually in the brain | Headache, confusion, lethargy, muscle weakness (in the arms, legs, or face), and seizures | |
Disseminated TB is associated with AIDS while pulmonary TB can occur in any stage of HIV infection | Cough, fevers, night sweats, weight loss, and chest pain | |
Infection of the intestine or lungs with bacteria that resemble tuberculosis bacteria | Fever, weight loss, diarrhea, and cough | |
Infection of the intestine with the parasite Cryptosporidium | Diarrhea, abdominal pain, and weight loss | |
Infection of the tissues covering the brain with the yeast Cryptococcus | Headache, fever, and confusion | |
Infection of the eyes or intestinal tract with cytomegalovirus | Eye: Clouding of vision or blindness Intestinal tract: Diarrhea and weight loss | |
Mpox (formerly monkeypox) | Infection with the mpox virus | Painful rash can begin in mouth or genitals then spread |
Saratani za kawaida kwa watu walio na maambukizi ya virusi vya Ukimwi
Kaposi sarcoma, a cancer caused by a sexually transmitted herpesvirus, appears as painless, red to purple, raised patches on the skin. It occurs mainly in men who have sex with men.


Image courtesy of Sol Silverman, Jr., via the Public Health Image Library of the Centers for Disease Control and Prevention.
Cancers of the immune system (lymphomas, typically non-Hodgkin lymphoma) may develop, sometimes first appearing in the brain. When the brain is affected, these cancers can cause weakness of an arm or a leg, headache, confusion, or personality changes.
Having HIV increases the risk of other cancers. They include cancer of the cervix, anus, testes, and lungs as well as melanoma and other skin cancers. Men who have sex with men are prone to developing cancer of the rectum due to the same human papillomaviruses (HPV) that cause cancer of the cervix in women.
Kisababishaji cha kifo
Usually, death is caused by the cumulative effects of opportunistic infections or cancers, wasting, and/or dementia.
Utambuzi wa maambukizi ya virusi vya Ukimwi
Tests to detect antibodies to the HIV virus in a sample of blood or saliva
Tests to detect HIV RNA in a sample of blood
Early diagnosis of HIV infection is important because it makes early treatment possible. Early treatment enables infected people to live longer, be healthier, and be less likely to transmit HIV to other people.
Doctors usually ask about risk factors for HIV infection (such as possible exposure in the workplace, high-risk sexual activities, and use of injected street drugs) and about symptoms (such as fatigue, rashes, and weight loss).
Doctors also do a complete physical examination to check for signs of opportunistic infections, such as swollen lymph nodes and white patches inside the mouth (indicating thrush), and for signs of Kaposi sarcoma of the skin or mouth.
Vipimo vya kutambua na kuchunguza
If doctors suspect exposure to HIV infection, they do a screening test for HIV. Doctors also offer a screening test to all adults and adolescents, particularly pregnant women early on in each pregnancy, regardless of what their risk appears to be. Anyone who is concerned about being infected with HIV can request to be tested. Such testing is confidential and often free of charge.

The current (fourth-generation) combination screening test tests for 2 things that suggest HIV infection:
Antibodies to HIV
HIV antigens (p24 antigen)
Antibodies are proteins produced by the immune system to help defend the body against a particular attack, such as that by HIV. Antigens are foreign substances that can trigger an immune response.
The body takes several weeks to produce enough antibodies to be detected by the test, so results of the antibody test are negative during the first few weeks after the virus enters the body (known as the "window period" of acute HIV infection). However, results of the p24 antigen test can be positive as early as 2 weeks after the initial infection. The combination tests can be done quickly by a laboratory. Also, a version of these tests can be done in a doctor's office or clinic (called bedside testing). If results are positive, doctors do a test to distinguish HIV-1 from HIV-2 and a test to detect the amount of HIV RNA in the blood (the viral load).
The combination screening test is quicker and less complex than older screening tests, which use enzyme-linked immunosorbent assay (ELISA) to detect HIV antibodies and then confirm positive results using a separate, more accurate, specific test such as the Western blot test. The Western blot test is expensive because it requires well-trained technicians and takes from several days to several weeks for results to be available. Most settings now use a special test called an HIV-1/HIV-2 differentiation assay (rather than the Western blot) to confirm an initial positive test result.
Other, older rapid bedside tests are also available. These tests can be done using a sample of blood or saliva. If results of these rapid screening tests are positive, they are confirmed by ELISA (with or without Western blot) or by repetition of one or more other rapid tests.
If people at low risk have a negative test result, the screening test is not repeated unless their risk status changes. If people at the highest risk have a negative test result (especially if they are sexually active, have several sex partners, or do not practice safer sex), testing should be repeated every 6 to 12 months.
HIV RNA tests can confirm positive results of an antibody test or detect evidence of HIV infection when antibody test results are negative. HIV RNA tests often use techniques to produce many copies of an organism's genetic material (called nucleic acid amplification). These tests can detect very small amounts of HIV RNA in blood and are very accurate.
Ufuatiliaji
If HIV infection is diagnosed, blood tests should be done regularly to measure the following:
CD4 count
Viral load
If the CD4 count is low, people are more likely to develop serious infections and other complications of HIV such as certain cancers. Viral load helps predict how fast the CD4 count is likely to decrease over the next few years.
These 2 measurements help doctors determine
How soon to start antiretroviral medications
What effects treatment is likely to have
Whether other medications may be needed to prevent complicating infections
With successful treatment, the viral load falls to very low levels within weeks, and the CD4 count begins a slow recovery toward normal levels.
Utambuzi wa UKIMWI (maambukizi ya VVU ya mwisho)
AIDS is diagnosed when the CD4 count falls below 200 cells per microliter of blood or when extreme wasting or certain serious opportunistic infections or cancers develop.
Utambuzi wa hali zinazohusiana na VVU
Various tests may be done to check for conditions that can accompany HIV infection. These tests include the following:
Bone marrow aspiration and biopsy: To further evaluate low blood cell counts (including anemia), which may be due to lymphomas, cancers, and opportunistic infections
Computed tomography (CT) with a contrast agent or magnetic resonance imaging (MRI): To check for damage to the brain or spinal cord
Matibabu ya Maambukizi ya Virusi Vya Ukimwi
Antiretroviral medications
Sometimes medications to prevent opportunistic infections
Sometimes medications to relieve symptoms
(See also Antiretroviral Treatment of HIV Infection.)
Treatment with antiretroviral medications is recommended for all people with HIV infection because without treatment, HIV infection can lead to serious complications and because newer, less toxic medications have been developed. For most people, early treatment has the best results. Research has shown that people who are promptly treated with antiretroviral medications are less likely to develop HIV/AIDS-related complications and to die of them.
Treatment cannot eliminate the virus from the body, although the HIV level often decreases so much that it cannot be detected in blood or other fluids or tissues. The goals of treatment are
Reducing HIV level to undetectable
Restoring CD4 count to normal
If treatment is stopped, the HIV level increases, and the CD4 count begins to fall. Thus, people need to take antiretroviral medications for their lifetime.
Before starting a treatment regimen, people are taught about the necessity of the following:
Taking medications as directed
Not skipping any doses
Taking the medications for the rest of their life
Taking the medications as directed for a lifetime is demanding. Some people skip doses or stop taking the medications for a time (called a drug holiday). These practices are dangerous because they enable HIV to develop resistance to the medications.
Because taking HIV medications irregularly often leads to drug resistance, health care practitioners try to make sure that people are both willing and able to adhere to the treatment regimen. To simplify the medication schedule and to help people take the medications as directed, doctors often prescribe treatment that combines 2 or more medications in 1 tablet that can be taken only once a day.
Uchanjaji
People with HIV infection should have the following vaccinations (for more information, see Centers for Disease Control and Prevention [CDC] immunization recommendations):
Conjugate pneumococcal vaccine PCV20 alone, or PCV15 followed by PPSV23 at least 8 weeks later, if they have not had a conjugate pneumococcal vaccine before
Influenza vaccine every year
Hepatitis B vaccine if they have not had the vaccine before or have not completed the series of 3 vaccinations
Hepatitis A vaccine if they are at increased risk of or desire protection from hepatitis A
Human papillomavirus (HPV) vaccine to prevent HPV-related mouth and throat, cervical, penile, and anal cancers (given to females and males at the recommended ages)
Meningococcal vaccine if adults have not had the vaccine before (doses are given at least 8 weeks apart and readministered every 5 years)
Tetanus-diphtheria vaccine (Td) with a booster every 10 years. People who have not received or completed a primary vaccination series of at least 3 doses of tetanus and diphtheria vaccine should begin or complete the series, and tetanus-diphtheria-pertussis vaccine (Tdap) should be substituted for one of the Td boosters if they have never received Tdap. People who have completed a primary series but have not previously received the Tdap, should receive Tdap for their next Td booster.
Varicella vaccine, in certain people with a CD4 count greater than 200 cells per microliter of blood
COVID-19 vaccine, regardless of CD4 count or viral load, because the potential benefits outweigh potential risks
Mpox vaccine for those at risk for mpox
Pregnant women with HIV should receive the routine vaccines recommended during pregnancy.
Ubashiri wa Maambukizi ya Virusi Vya Ukimwi
Exposure to HIV does not always lead to infection, and some people who have had repeated exposures over many years remain uninfected. Moreover, many people who are treated with antiretroviral medications can manage HIV infection as a chronic illness, without developing AIDS. With effective treatment, the HIV RNA level decreases to undetectable levels, CD4 counts increase significantly, and people can continue to lead productive, active lives. The risk of illness and death decreases but remains higher than that of people who are of similar age and who are not infected with HIV. However, if people cannot tolerate or take medications consistently, HIV infection and immune deficiency progresses, causing serious symptoms and complications.
Many untreated people with HIV infection remain well for more than a decade. A very few untreated people have remained well for over 20 years. Why some people become ill so much sooner than others is not fully understood, but a number of genetic factors appear to influence both susceptibility to infection and progression to AIDS after infection.
If infected people are not treated, AIDS develops in most of them. How quickly the number of CD4 cells decreases and HIV infection progresses toward AIDS varies greatly from person to person. Generally, experts estimate that if untreated, people develop AIDS at the following rates:
For the first several years after infection: 1 to 2% each year
Each year thereafter: 5 to 6%
Within 10 to 11 years: 50%
Eventually: More than 95%, possibly all if they live long enough
Usually, HIV infection does not directly cause death. Instead, HIV infection leads to a substantial loss of weight (wasting), opportunistic infections, cancers, and other disorders, which then lead to death.
Cure has been thought to be impossible, although intensive research on how to eliminate all of the latent HIV from infected people continues.
Masuala ya mwisho wa uhai
Because death rarely occurs suddenly in people with AIDS, people usually have time to make plans for the kind of health care they want if their condition worsens. Nonetheless, people should record such plans in a legal document early and should include clear instructions about the kind of care they want (called advance directives).
Near the end of life, many people have pain and other distressing symptoms (such as agitation) and usually lose their appetite. In high-income countries, hospice programs are particularly equipped to deal with such problems. They can provide comprehensive support and care, which focuses on managing symptoms, helping dying people maintain their independence, and supporting their caregivers.
Kinga ya Maambukizi ya Virusi vya Ukimwi
At present, there is no effective HIV vaccine to prevent HIV infection or slow its progression in people who are already infected. However, treating people who have HIV infection reduces the risk of their transmitting the infection to other people.
Transmission of HIV through its most common routes—sexual contact or sharing of needles—is almost completely preventable. However, the measures required for prevention—sexual abstinence or consistent condom use and access to clean needles—are sometimes personally or socially unpopular. Many people have difficulty changing their addictive or sexual behaviors, so they continue to put themselves at risk of HIV infection. Also, safer sex practices are not foolproof. For example, condoms can leak or break.
Condoms made of latex provide good protection against HIV (as well as other common sexually transmitted infections), but they are not foolproof. Oil-based lubricants (such as petroleum jelly) should not be used because they may dissolve latex, reducing the condom's effectiveness.
Other measures can help. For men, circumcision, an inexpensive, safe procedure, reduces the risk of becoming infected during vaginal intercourse with an infected woman by about half. Whether circumcision reduces the risk of HIV infection in other circumstances is unclear. Because circumcision provides only partial protection against HIV infection, people should also use other measures to prevent HIV infection. For example, if either partner has a sexually transmitted infection or HIV infection, it should be treated, and condoms should be used correctly and consistently.
Tahadhari za Ulimwengu
People who are likely to come into contact with blood or other body fluids at their job should wear protective latex gloves, masks, and eye shields. These precautions apply to body fluids from all people, not just those from people with HIV, and are thus called universal precautions. Universal precautions are taken for 2 reasons:
People with HIV may not know that they are infected.
Viruses that cause other serious disorders (such as hepatitis B and C) can be transmitted by body fluids.
Surfaces contaminated with HIV can easily be cleaned and disinfected because HIV is inactivated by heat and by common disinfectants such as hydrogen peroxide and alcohol.
Because HIV is not transmitted through the air or by casual contact (such as touching, holding, or dry kissing), hospitals and clinics do not isolate people with HIV infection unless they have another contagious infection.
Kuzuia usambazaji kwa kuongezewa damu na vipandikizi vya kiungo
In the United States, the following have almost eliminated transmission of HIV infection by organ transplantation or blood transfusion:
Screening donors of organs or blood for risk factors for HIV infection
Screening donated blood for HIV
Risk is reduced further by asking people with risk factors for HIV infection, regardless of their test results for HIV, to not donate blood or organs for transplantation. The Red Cross has issued guidance for deferral of blood donation, including deferral for having
Had a new sex partner in the last 3 months
Had more than 1 sex partner in the last 3 months
Engaged in anal sex in the last 3 months
However, low-resource countries have not consistently used sensitive HIV screening tests and have not restricted donors. Consequently, transmission by these routes is still a problem in these countries.
Kuzuia maambukizi kutoka kwa mama hadi mtoto aliyezaliwa karibuni
Pregnant women infected with HIV can transmit the virus to the newborn.
The following can help prevent HIV transmission from mother to newborn:
Testing pregnant women early in each pregnancy to determine whether they are infected with HIV
If they are infected, treating them with antiretroviral medications during pregnancy and labor (treatment during labor is especially important)
Delivering the baby by cesarean rather than by vaginal delivery
After birth, treating the newborn with zidovudine, given intravenously, for 6 weeks
If possible, using formula instead of breastfeeding (HIV can be transmitted in breast milk)
Matibabu ya kuzuia kabla ya mfichuo
Taking an antiretroviral medication before being exposed to HIV can reduce the risk of HIV infection. Such preventive treatment is called preexposure prophylaxis (PrEP). However, PrEP is expensive and is effective only if people take the medication every day. Thus, PrEP is recommended only for people who have a very high risk of becoming infected, such as people who have a partner who is infected with HIV, people who have sexual behaviors that place them at substantial risk of HIV infection, and people who inject drugs and have injection practices that place them at substantial risk of HIV infection.
PrEP may also be recommended for people who engage in high-risk sexual activities, such as the following:
Men who have anal sex with men without using a condom
Heterosexual men and women who do not regularly use condoms during sex with partners whose HIV status is unknown and who are at increased risk of HIV infection
People who use PrEP still need to use other methods to prevent HIV infection, including consistent use of condoms and not sharing needles to inject drugs.
Matibabu ya kuzuia baada ya mfichuo
The policies and procedures used to help decrease the risk of infection after exposure to HIV is called postexposure prophylaxis (PEP). People who have been exposed to HIV from a blood splash, needlestick, or sexual contact may reduce the chance of infection by taking antiretroviral medications for 4 weeks. These medications are more effective when they are started as soon as possible after the exposure. Taking 2 or more medications is currently recommended.
Doctors and the person who was exposed typically decide together whether to use these preventive medications. They base the decision on the estimated risk of infection and the possible side effects of the medications. If they do not know whether the source is infected with HIV, they consider how likely the source is to be infected. However, even when the source of the exposure is known to be infected with HIV, the risk of infection after exposure varies, depending on the type of exposure. For example, risk from a blood splash is less than that from a needlestick.
Immediately after exposure to HIV infection, what is done depends on the type of exposure:
If skin is exposed, it is cleaned with soap and water.
Puncture wounds are cleaned with antiseptic.
If mucous membranes are exposed, they are flushed with large amounts of water.
Taarifa Zaidi
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
Office of AIDS Research: Information from the National Institutes of Health (NIH), including a glossary of HIV-related terms and a drug database
Centers for Disease Control and Prevention (CDC) 2024 Immunization Schedule: Recommended adult immunization schedule by medical condition and other indications
CDC: Post-Exposure Prophylaxis (PEP): Resources regarding the use of antiretroviral medications after a single high-risk event to stop HIV
The American Foundation for AIDS Research: Resources regarding the support of AIDS research, HIV prevention, treatment education, and advocacy
American Sexual Health Association: Information about sexual health
Centers for Disease Control and Prevention (CDC): HIV/AIDS: General information about HIV/AIDS, including information on home testing and risk reduction tools
Gay Men's Health Crisis: General information on men's health, including HIV testing


